
Clinical Case of Feline Corneal Sequestrum in a 4-year-old Cat
This article shares a clinical case of feline corneal sequestrum in a 4-year-old Persian cat. The affected cat had a black area on its right cornea for one to two years and sought veterinary attention after symptoms such as eye redness emerged.
In this case, the cat’s corneal sequestrum was successfully resolved through a combination of surgical and medical treatment. Post-operatively, high corneal transparency and good ocular aesthetics were achieved. During subsequent follow-ups, new symptoms were addressed with eyelid entropion correction, cryoepilation of abnormal hairs, and lamellar keratectomy on the left eye. This case highlights the importance of early, comprehensive treatment for feline corneal sequestrum, along with the necessity of identifying and addressing the underlying cause. The diagnostic and treatment process for this case is organized below for your reference.
Affected Animal Information
Here’s the information about the affected animal:
- Animal Type: Cat
- Breed: Persian
- Age: 4 years old
- Sex: Male
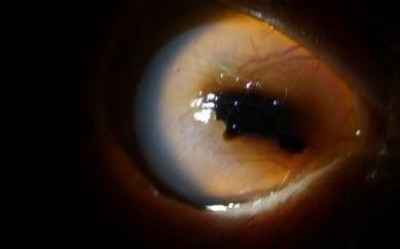
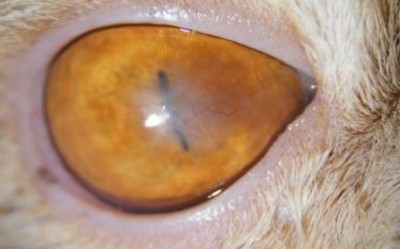
- Chief Complaint: On May 21, 2023, the cat’s right eye had a black corneal area for one to two years. Recently, the eye became red, the cornea significantly cloudy, and there was tearing.
- Reason for Consultation: Significant tearing and pain, with recent noticeable corneal cloudiness. The owner was concerned about worsening of the condition.
Clinical Signs
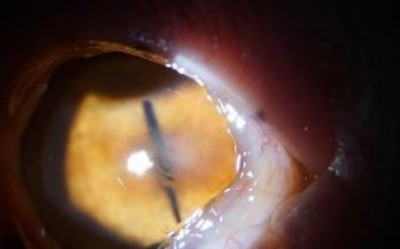
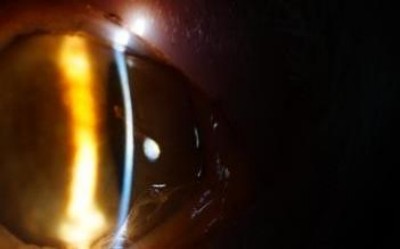
- Right Eye: Eyelid redness, conjunctival hyperemia and swelling, corneal edema and cloudiness, extensive neovascularization, large area of cornea turned black, poor light transmission visible on slit lamp examination, anterior chamber flare (+).
- Both Eyes: Entropion of the lower eyelid at the medial canthus.
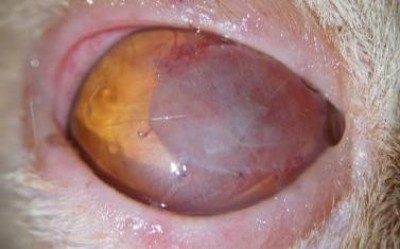
- Left Eye: Cornea became yellowish-brown from the 8 o’clock to 9 o’clock position.
Check up
Ophthalmic Testing
| Examination Item | OD | OS |
| STT, mm/min | 22 | 15 |
| IOP, mmHg | 11 | 16 |
| Menace / Dazzle | +/+ | +/+ |
| Palpebral / Corneal | +/+ | +/+ |
| PLR | +/+ | +/+ |
| Fluorescein | + | – |
Slit lamp examination





OD OS
Fluorescein
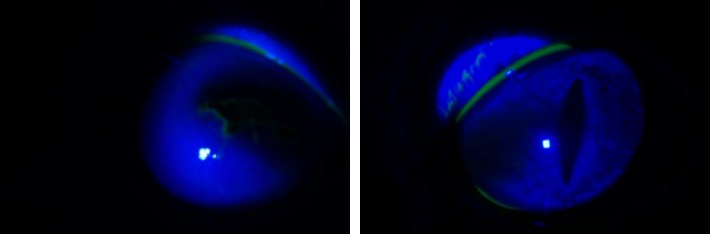
OD OS
Tentative Diagnosis
OU Entropion, Corneal Sequestrum
Item |
Unit |
Actual Value |
Reference Rang |
| RBC | x10^12/L | 4.7 | 6.54-12.20 |
| HCT | % | 47.9 | 30.3-52.3 |
| HGB | g/dL | 15.3 | 9.8-16.2 |
| MCV | fL | 36.7 | 35.9-53.1 |
| MCH | pg | 12 | 11.8-17.3 |
| MCHC | g/dL | 32.6 | 28.1-35.8 |
| RDW | % | 30.5 | 15.0-27.0 |
| RETIC | % | 0.3 | – |
| RETIC | K/μL | 34.5 | 3.0-50.0 |
| RETIC-HGB | pg | 14.5 | 13.2-20.8 |
| WBC | x10^9/L | 10.27 | 2.87-17.02 |
| NEU % | % | 32.7 | – |
| LYM % | % | 55.8 | – |
| MON % | % | 2 | – |
| EOS % | % | 8.2 | – |
| BASO % | % | 1.3 | – |
| NEU | x10^9/L | 3.36 | 2.30-10.29 |
| LYM | x10^9/L | 5.73 | 0.92-6.88 |
| MON | x10^9/L | 0.21 | 0.05-0.67 |
| EOS | x10^9/L | 0.84 | 0.17-1.57 |
| BASO | x10^9/L | 0.13 | 0.01-0.26 |
| PLT | K/μL | 89 | 151-600 |
| MPV | fL | 20 | 11.4-21.6 |
| PC | % | 0.18 | 0.17-0.86 |
| GLU | mmol/L | 5.79 | 4.11-8.84 |
| CREA | μmol/L | 127 | 71-212 |
| UREA | mmol/L | 7.4 | 5.7-12.9 |
|
BUN/CREA ratio
|
14 | – | |
| PHOS | mmol/L | 1.9 | 1.00-2.42 |
| CA | mmol/L | 2.46 | 1.95-2.83 |
| TP | g/L | 74 | 57-89 |
| ALB | g/L | 35 | 22-40 |
| GLOB | g/L | 39 | 28-51 |
| A/G | 0.9 | – | |
| ALT | U/L | 52 | 12-130 |
| ALP | U/L | 36 | 14-111 |
| GGT | U/L | 0 | 0-4 |
| TBIL | μmol/L | <2 | 0-15 |
| CHOL | mmol/L | 4.58 | 1.68-5.81 |
Treatment Plan
Medical Treatment:
- Topical Medication: Ofloxacin eye drops with serum, 1 hour/time; Sodium hyaluronate, 1 hour/time.
- Systemic Medication: Systemic use of analgesic and anti-inflammatory drugs, such as Meloxicam; Oral antiviral medication, Famciclovir, 90 mg/kg.
Surgical Intervention:
Consider surgical treatment options: excision of the right eye’s corneal nigra (or corneal sequestrum) combined with artificial corneal patch graft.
- Preoperative Preparation: Comprehensive examination, anesthesia evaluation.
- Surgical Procedure: Complete excision of the discolored cornea under an ophthalmic operating microscope, creation of a circular recipient bed, trimming the artificial corneal patch to an appropriate size, and suturing it securely onto the recipient bed.
Key Step: Complete excision of the discolored cornea is required during surgery.
Treatment Outcome and Follow-up
Postoperative Outcome:
1-week follow-up after surgery: Mild conjunctival swelling in the right eye, secure adhesion between the corneal patch and the corneal recipient bed, stable corneal sutures, and neovascularization growing around the patch. The discoloration of the left cornea remains largely unchanged.

OD OS
1-month follow-up after surgery: Conjunctival swelling in the right eye has resolved, the corneal patch has undergone some absorption with reduced area, neovascularization continues to grow towards the central cornea, and corneal sutures remain stable. The discoloration of the left cornea remains largely unchanged.

OD OS
2-month follow-up after surgery: Conjunctiva in the right eye is normal, the corneal patch has completely absorbed, a faint white scar tissue is present in the central cornea, with a small amount of neovascularization, and corneal sutures have absorbed and disappeared. The discoloration of the left cornea remains largely unchanged.

OD OS
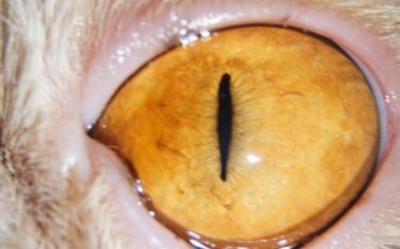
3-month follow-up after surgery: The original scar tissue in the central cornea has faded, and corneal transparency has increased. The discoloration of the left cornea has improved, and transparency has increased.


OD OS
Follow-up Plan: Recheck every 2-3 months to observe changes in the corneas of both eyes.
On July 14, 2024, both eyes presented with inability to open, redness and swelling, and tearing. After slit lamp examination, it was found that the right eye had conjunctival redness and swelling, with a band-like brownish area appearing in the central cornea and increased neovascularization. The left eye had conjunctival redness and swelling, with the original corneal nigra (or corneal sequestrum) area worsening, becoming darker in color and increasing in scope, and the center of the corneal nigra area turning black. The entropion of the medial lower eyelids in both eyes remained. Based on the band-like brownish area in the right cornea, it was suspected that there might be an issue with incomplete eyelid closure. Upon careful observation by the owner, it was discovered that the cat’s eyelids did not completely close during sleep.




OD OS
Treatment Plan: Bilateral medial lower eyelid entropion correction combined with cryotherapy for abnormal hairs. Left eye to undergo lamellar keratectomy. Postoperatively, both eyes to use antibiotic eye drops and corneal repair eye drops. The right eye to use long-acting moisturizing eye drops before sleep.
Postoperative Outcome: Entropion improved, no hair irritation to the ocular surface, and increased corneal transparency in both eyes.


OD OS
Follow-up Plan: Recheck every 2-3 months to observe changes in the corneas of both eyes.
Treatment Outcome and Follow-up
Case Summary: This case demonstrates the diagnosis and treatment plan for feline corneal sequestrum (or corneal nigra). Through a combination of surgery and medication, the disease was successfully resolved, resulting in high corneal transparency and good ocular aesthetics postoperatively.
Treatment Insights:
For corneal sequestrum (or corneal nigra), comprehensive treatment should be initiated as early as possible to avoid delaying the condition. The optimal treatment for corneal sequestrum is surgical intervention, involving the excision of the discolored necrotic cornea and corneal grafting. The specific method of corneal grafting should be chosen based on the necrotic area, depth, and the owner’s expectations. After complete corneal recovery, a white scar will form at the surgical site, with the color of the scar varying due to the depth of excision and individual animal differences. To treat corneal sequestrum, it is crucial to identify the underlying cause and provide targeted treatment accordingly. For instance, in this case, it was highly suspected that the bilateral corneal sequestrum was caused by entropion of the lower eyelids with abnormal hair irritating the ocular surface.
This was supported by the central and medial location of the corneal nigra in both eyes. Therefore, the treatment plan not only addressed the corneal sequestrum but also rectified the entropion and the issue of abnormal hair irritation. The recurrence of corneal sequestrum in the right eye strongly suggested an issue with incomplete eyelid closure, leading to chronic dryness of the central cornea and subsequent corneal nigra due to chronic inflammatory stimulation. This was supported by the central and band-like appearance of the right corneal nigra. Long-term ocular surface hydration is therefore essential.